Healthcare AI Intake Had Its Infrastructure Week
Three separate healthcare AI intake launches in 48 hours reveal a shift: front-office automation is becoming platform infrastructure, not a chatbot layer.
By Springvanta
Something shifted this week in healthcare AI, and it happened fast enough that you could miss it if you weren't watching.
Between Tuesday and Wednesday, three organizations published details about AI-powered front-office and intake systems. Not chatbots. Not pilot programs with three doctors. Actual production-grade deployments at scale: a public SaaS company, a top-five academic health system, and AWS. Different buyers, different tech stacks, different go-to-market motions. The same bet on the same workflow.
Here is what shipped, and why the convergence matters more than any individual announcement.
Penn Medicine bet on AI intake as core infrastructure
On May 27, the University of Pennsylvania Health System announced a multi-year partnership with K Health to deploy clinical AI agents directly inside its EHR systems and patient portals. Not a standalone symptom checker living on a website somewhere. Not a chatbot widget. The agents are integrated into the electronic health record and the public-facing digital front door, starting with Penn Medicine On-Demand (virtual urgent care) before expanding to primary care, cardiology, and dermatology.
The intake experience itself is worth noting. When a patient requests care, the K Health agent opens a conversational dialogue, not a static form. It asks follow-up questions based on what the patient describes. It translates symptoms, medications, and care history into structured medical data. Then it pre-populates a draft clinical chart that appears in the physician's EHR before the visit begins.
Ran Shaul, K Health's co-founder and chief product officer, framed it as "foundational infrastructure" rather than a feature. Penn Medicine is treating clinical AI the way it treats its EHR: something that has to work at system scale, not a departmental experiment.
Penn Medicine and K Health are also planning peer-reviewed research on how autonomous agents affect workflow efficiency and patient compliance over time. That matters. Most healthcare AI announcements skip the evidence-building part entirely.
Weave built an omnichannel AI receptionist on Google Gemini
The next day, May 28, Weave (NYSE: WEAV) launched its Omnichannel AI Receptionist, built on Google Cloud's Gemini Enterprise Agent Platform. Weave serves over 40,000 healthcare practice locations and processes more than a billion patient interactions annually. This is not a startup looking for product-market fit.
The receptionist handles voice and text conversations, preserves context when a patient switches channels (say, from a phone call to SMS), and routes complex requests to live staff. It is embedded in Weave's existing front-office platform, not sold as a separate product. Practices configure how the AI fits into their call flows and when it should hand off to a human.
Weave's Q1 2026 earnings (reported April 30) give context for where this sits in the business. Revenue hit $65.5 million, up 17.4% year over year. Over 50% of customer locations already use at least one embedded AI feature. Platform-handled AI interactions grew more than 300% year over year. The AI receptionist is being monetized through a hybrid subscription and consumption model tied to usage.
One in three calls to dental offices are missed during business hours, according to Weave's data. That stat alone explains why an always-on AI receptionist that books appointments and handles insurance questions has clear ROI for a small practice.
AWS published the engineering details behind Amazon Connect Health
Also on May 27, AWS published a deep technical blog on how it built Amazon Connect Health, its agentic healthcare solution that launched in March 2026. The post is unusually detailed for a vendor engineering blog, and the specifics tell you where enterprise healthcare AI intake is heading.
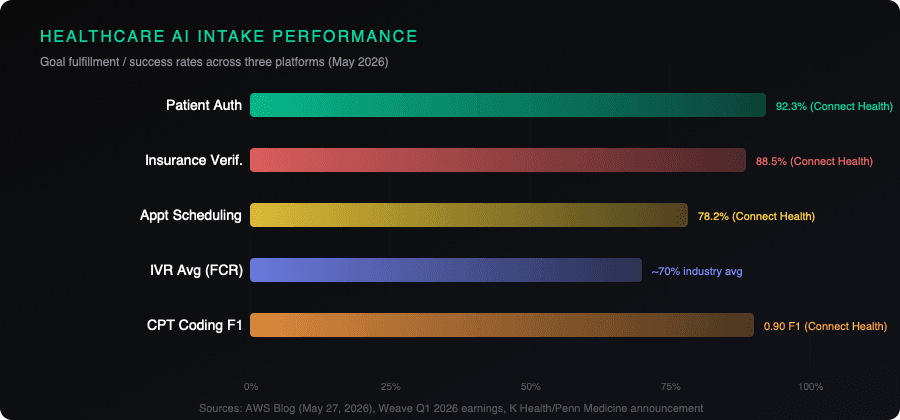
Connect Health covers five workflows: pre-visit patient insights, ambient clinical documentation during the visit, post-visit medical coding, and two patient-facing capabilities (authentication and appointment scheduling via voice agents).
The patient engagement agents replace traditional IVR systems with natural language conversations integrated with EHRs. The voice agent authenticates patients (92.3% success rate), verifies insurance (88.5% goal fulfillment), and schedules appointments (78.2% goal fulfillment). These numbers benchmark against an IVR industry average of roughly 70% first-call resolution. After three failed attempts, the agent transfers to a human.
On the clinical side, AWS fine-tuned smaller language models (under 10B parameters) that outperformed larger foundation models: 2.2x faster generation, 50% fewer documentation issues, 180x lower cost, and 35% shorter notes while preserving clinical completeness. The medical coding model (trained jointly on ICD and CPT codes) achieved 0.89 F1 on ICD and 0.90 F1 on CPT against proprietary data. On the public ACI-Bench dataset, it scored 0.69 F1 compared to 0.39 for a simple LLM prompt and 0.52 for chain-of-thought with extended thinking.
AWS used multi-stage reinforcement learning (GRPO) to get small models to match or exceed supervised fine-tuning alone. The key finding: combining all reward functions in a single RL step did not beat the SFT model. Separating rewards into sequential stages, each optimizing one objective, did. That is a useful data point for anyone building domain-specific AI agents.
Why three launches in 48 hours matters
None of these three organizations coordinated. They serve different segments (academic medical centers, small-to-mid-size practices, enterprise cloud customers). They use different underlying models (K Health's proprietary clinical models, Google Gemini, AWS's fine-tuned small models). They announced within 48 hours of each other.
The shared pattern is the real story.
All three treat the patient intake and front-office workflow as platform infrastructure, not a feature add-on. All three embed AI into existing systems (EHR, practice management, contact center) rather than asking staff to adopt a new interface. All three handle the full patient journey: scheduling, intake, documentation, and billing. And all three build in escalation to humans rather than pretending AI can handle everything.
This is the "infrastructure phase" of healthcare AI intake. The chatbot-in-a-widget era is ending. What replaces it is a conversational intake layer woven into the systems staff already use, with guardrails, audit trails, and evidence mapping baked in.
For practice operators and health system CIOs, the practical takeaway is straightforward: the question is no longer whether to deploy AI intake. It is whether to buy it embedded in your existing platform (Weave, your EHR vendor) or build it on cloud infrastructure (AWS, K Health). The first option is faster. The second gives you more control. Both are now production-ready.
If you are evaluating AI intake for your practice or health system, the specs that matter most from this week's announcements are: conversational (not form-based) intake, pre-populated clinical charts, context preservation across channels, configurable escalation rules, and peer-reviewed evidence (or at minimum, published benchmarks). If a vendor cannot show you at least three of those five, they are selling last year's product.
Sources
- K Health and Penn Medicine announce AI collaboration (BusinessWire, May 27, 2026): https://www.businesswire.com/news/home/20260527013277/en/K-Health-and-Penn-Medicine-Announce-AI-Collaboration-to-Support-Patient-Intake
- Penn Medicine deploys K Health clinical AI (HIT Consultant, May 27, 2026): https://hitconsultant.net/2026/05/27/penn-medicine-deploys-k-health-clinical-ai/
- Penn Medicine, K Health partner to deploy AI clinical agents (Fierce Healthcare, May 27, 2026): https://www.fiercehealthcare.com/ai-and-machine-learning/penn-medicine-k-health-partner-deploy-clinical-ai-clinical-agents
- Weave unveils omnichannel AI receptionist built with Google Gemini (BusinessWire via FT, May 28, 2026): https://markets.ft.com/data/announce/detail?dockey=600-202605280800BIZWIRE_USPRX____20260528_BW982874-1
- Weave Q1 2026 earnings call transcript (SEC filing, April 30, 2026): https://www.sec.gov/Archives/edgar/data/1609151/000160915126000046/a991-weaveearningsreleasex.htm
- How we built healthcare AI you can trust: Amazon Connect Health (AWS Blog, May 27, 2026): https://aws.amazon.com/blogs/industries/how-we-built-healthcare-ai-you-can-trust-the-engineering-behind-amazon-connect-health/